0
Skip to Content
Home
Our Services
Our Story
Contact Us
Book Services
Open Menu
Close Menu
Home
Our Services
Our Story
Contact Us
Book Services
Open Menu
Close Menu
Home
Our Services
Our Story
Contact Us
Book Services
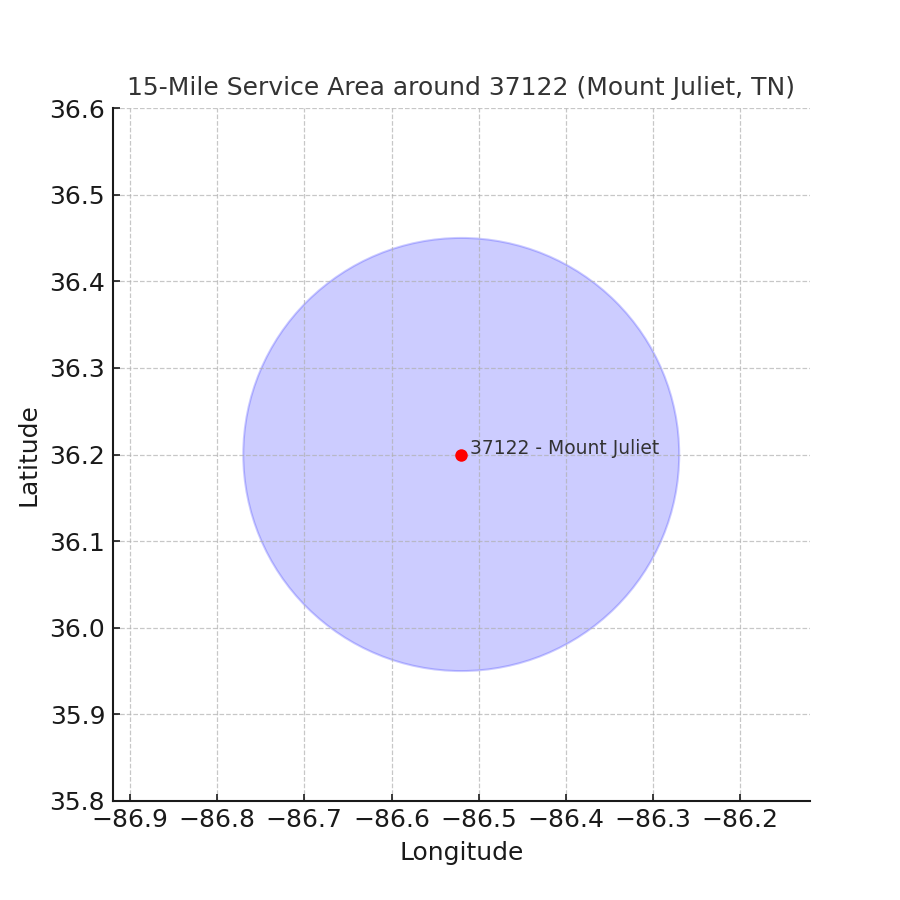
Service Area